— OPINION —
Famous Anthony’s “About Us” Page in its website tells the story of a family run, Roanoke institution that has been taken to its knees in bankruptcy because one employee was not vaccinated against hepatitis A. Sadder still are the 50 customers sickened, some so severely that they required liver transplants, and in four instances they died, including two members of one family.
The “About Page” says:
We are often asked what makes us famous. We’ve always been known for our food and service, but to us, it’s our customer (you!) that makes us famous. Since 1986 we’ve been an integral part of the community and our story has been woven by our customers, spanning many generations of families. It’s their stories that makes ours.
We are still family owned and operated and you can often find Mr. Anthony out and about in the restaurants. So come by and give us a visit. As our customers say, visit once and you’re family.”
My guess is that Mr. Anthony wishes that he had taken the About Page to heart and protected his family by offering vaccinations to all employees or seeking free vaccines from the local health department. But, he did not and now it is too late for many customers and for his 40 year old business.
An outbreak of hepatitis A occurred in the early fall of 2021 in Roanoke City, Virginia. The health department was notified about the outbreak on September 21, 2021, after the first case was reported by a local hospital. The Roanoke City Health Department, along with the Virginia Department of Health, investigated this outbreak. Three different Famous Anthony’s locations were ultimately found associated with this outbreak: 6499 Williamson Road, Roanoke; 4913 Grandin Road, Roanoke; and 2221 Crystal Springs Avenue, Roanoke. A public posting was made by the Virginia Department of Health on September 24, 2021, about this outbreak and the potential exposure risk.
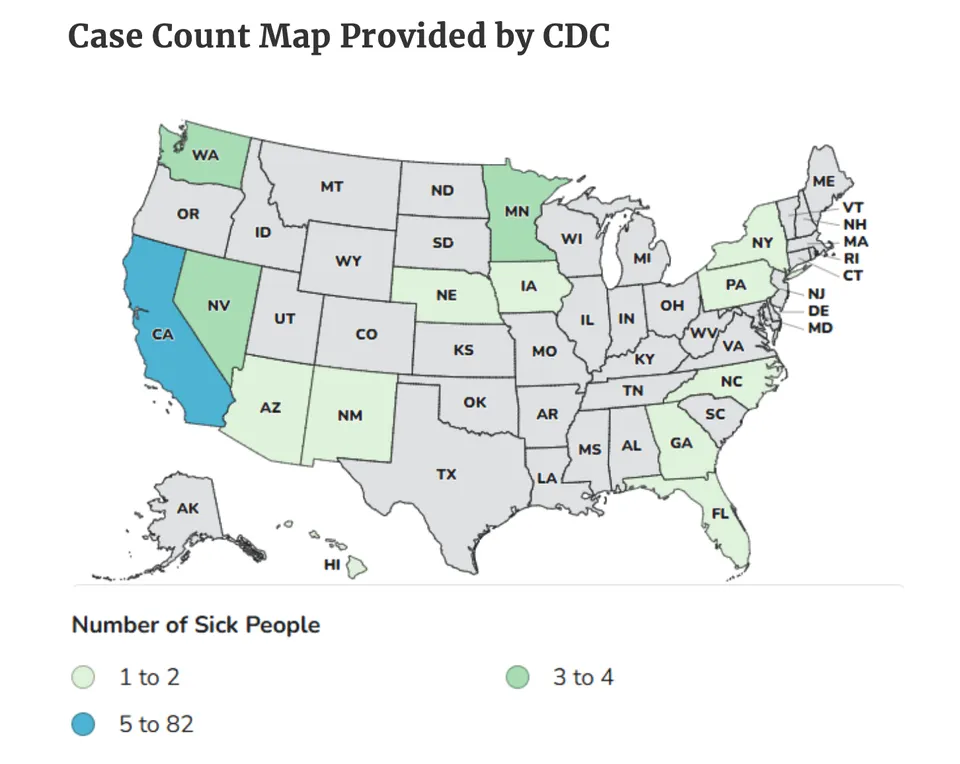
As of November 2021, a total of 52 primary cases (41 confirmed and 11 probable) were identified in this outbreak. Two secondary cases were also identified. Cases ranged from 30 to 82 years of age (median 63). In all, 57 percent of cases were male. Thirty-three cases included hospitalizations, and at least 4 cases involved deaths. Exposures to the Famous Anthony’s food establishments occurred between August 10 and 27, 2021. Illness onsets occurred between August 25 and October 15, 2021.
A cook, who also had risk factors associated with hepatitis A, was found to be infected with hepatitis A while working at multiple Famous Anthony’s restaurant locations. This index case’s mother and adult son also tested positive for hepatitis A. Following an inspection, the inspector noted, “due to the etiology of Hepatitis A transmission, it is assumed the infectious food handler did not perform proper hand washing or follow glove use policy.” It was determined that person-to-person spread was the most likely mode of transmission in this outbreak. Environmental contamination was also considered a possible mode of transmission.
Exposure to hepatitis A virus (“HAV”) can cause an acute infection of the liver that is typically mild and resolves on its own.[1] The symptoms and duration of illness vary a great deal, with many persons showing no symptoms at all.[2] Fever and jaundice are two of the symptoms most associated with HAV infection.[3]
Hepatitis A is the only common vaccine-preventable foodborne disease in the United States.[4] This virus is one of five human hepatitis viruses that primarily infect the human liver and cause human illness.[5] Unlike hepatitis B and C, hepatitis A does not develop into chronic hepatitis or cirrhosis, which are both potentially fatal conditions.[6]Nonetheless, infection with the hepatitis A virus (HAV) can lead to acute liver failure and death.[7]
Hepatitis A is a communicable (or contagious) disease that often spreads from person to person.[8] Person-to-person transmission occurs via the “fecal-oral route,” while all other exposure is generally attributable to contaminated food or water.[9] Food-related outbreaks are usually associated with contamination of food during preparation by a HAV-infected food handler.[10] The food handler is generally not ill because the peak time of infectivity—that is, when the most virus is present in the stool of an infected individual—occurs two weeks before illness begins.[11]
According to Lin & Fang[12], the recent upsurgence of hepatitis A transmitted from person-to-person has raised alarm among public health officials. Although hepatitis A is primarily foodborne, hepatitis A virus (HAV) can also be transmitted through close contact. The authors point to increasing rates of person-to-person transmission of hepatitis A across the world since 2015, which international health organizations now recognize as a reemerging health threat.
In the United States, the increase in hepatitis A outbreaks from 2016 to the present are thought to be at least partially related to people using drugs and being homeless; however, both medical and nonmedical factors account for the observed increase of hospitalization and deaths. Of particular concern is the rising risk of morbidity during this wave of outbreaks. Recent studies cited by Lin & Fang show that more than half (52%) of patients were hospitalized, of whom 10% required intensive care, 4% developed fulminant hepatitis, and 1% died. This is in sharp contrast to past studies, where serious hepatic complications associated with acute hepatitis A were rarely reported. Nonetheless, these findings highlight the importance of HAV vaccinations for at-risk populations.
As recommended in the United States by the Advisory Committee on Immunization Practices (ACIP), from a public health perspective, HAV vaccination is the most effective prevention strategy to control a person-to-person transmitted hepatitis A outbreak. HAV vaccines are highly immunogenic, and >95% of immunocompetent individuals achieve seroconversion within 4 weeks after the first dose. Despite the benefits of vaccination, several barriers and missed opportunities to vaccination were identified from the experiences during the hepatitis A outbreaks. Hofmeister et. al[13]cite recent research describing that information on HAV vaccination status was missing in nearly two-thirds of study participants, and nearly 90% of those with available information had not previously received HAV vaccines. Citing another study reporting a hepatitis A outbreak in San Diego County, no hepatitis A case patients had ever received a full series of HAV vaccinations.
HAV is relatively stable and can survive for several hours on fingertips and hands, and up to two months on dry surfaces.[14] The virus can be inactivated by heating to 185°F (85°C) or higher for one minute or disinfecting surfaces with a 1:100 dilution of household bleach in tap water.[15] HAV can still be spread from cooked food if it is contaminated after cooking.[16]
Hepatitis A may cause no symptoms at all when it is contracted, especially in children.[17] Asymptomatic individuals will only know they were infected (and have become immune, given that you can only get hepatitis A once) by getting a blood test later in life.[18] Approximately 10 to 12 days after exposure, HAV is present in blood and is excreted via the biliary system into the feces.[19] Although the virus is present in the blood, its concentration is much higher in feces.[20] HAV excretion begins to decline at the onset of clinical illness, and decreases significantly by 7 to 10 days after onset of symptoms.[21] Most infected persons no longer excrete virus in the feces by the third week of illness. Children may excrete HAV longer than adults.[22]
Seventy percent of HAV infections in children younger than six years of age are asymptomatic; in older children and adults, infection tends to be symptomatic with more than 70% of those infected developing jaundice.[23] Symptoms typically begin about 28 days after contracting HAV but can begin as early as 15 days or as late as 50 days after exposure.[24] The symptoms include muscle aches, headache, anorexia (loss of appetite), abdominal discomfort, fever, and malaise.[25]
After a few days of typical symptoms, jaundice (also termed “icterus”) sets in.[26] Jaundice is a yellowing of the skin, eyes, and mucous membranes that occurs because bile flows poorly through the liver and backs up into the blood.[27] The urine will also turn dark with bile and the stool light or clay-colored from lack of bile.[28] When jaundice sets in, initial symptoms such as fever and headache begin to subside.[29]
In general, symptoms usually last less than two months, although 10% to 15% of symptomatic persons have prolonged or relapsing disease for up to 6 months.[30] It is not unusual, however, for blood tests to remain abnormal for six months or more.[31] The jaundice so commonly associated with HAV can also linger for a prolonged period in some infected persons, sometimes as long as eight months or more.[32] Additionally, pruritus, or severe “itchiness” of the skin, can persist for several months after the onset of symptoms. These conditions are frequently accompanied by diarrhea, anorexia, and fatigue.[33]
Relapse is possible with hepatitis A, typically within three months of the initial onset of symptoms.[34] Although relapse is more common in children, it does occur with some regularity in adults.[35] The vast majority of persons who are infected with hepatitis A fully recover, and do not develop chronic hepatitis.[36] Persons do not carry HAV long-term as with hepatitis B and C.[37]
Fulminant hepatitis A, or acute liver failure, is a rare but devastating complication of HAV infection.[38] As many as 50% of individuals with acute liver failure may die or require emergency liver transplantation.[39] Elderly patients and patients with chronic liver disease are at higher risk for fulminant hepatitis A.[40] In parallel with a declining incidence of acute HAV infection in the general population, however, the incidence of fulminant HAV appears to be decreasing.[41]
HAV infects the liver’s parenchymal cells (internal liver cells).[42] Once a cell has been penetrated by the viral particles, the hepatitis A releases its own toxins that cause, in essence, a hostile takeover of the host’s cellular system.[43] The cell then produces new viral components that are released into the bile capillaries or tubes that run between the liver’s parenchymal cells.[44] This process results in the death of liver cells, called hepatic necrosis.[45]
The fulminant form of hepatitis occurs when this necrotic process kills so many liver cells—upwards of three-quarters of the liver’s total cell count—that the liver can no longer perform its job.[46] Aside from the loss of liver function, fulminant hepatic failure can lead to encephalopathy and cerebral edema.[47] Encephalopathy is a brain disorder that causes central nervous system depression and abnormal neuromuscular function.[48] Cerebral edema is a swelling of the brain that can result in dangerous intracranial pressure.[49] Intracranial hypertensions leading to a brain stem death and sepsis with multiple organ failure are the leading causes of death in individuals with fulminant hepatic failure.[50]
[1] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” in Mandell, Douglas, & Bennett’s PRINCIPLES AND PRACTICE OF INFECTIOUS DISEASES, Fifth Edition, Chap. 161, pp. 1920-40 (2000); Mayo Clinic Staff, “Hepatitis A,” (last updated Sept 1, 2011). Articles available online at http://www.mayoclinic.com/health/hepatitis-a/DS00397.
[2] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1.
[3] Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[4] Id.; See also Fiore, Anthony, Division of Viral Hepatitis, CDC, “Hepatitis A Transmitted by Food,” Clinical Infectious Diseases, Vol. 38, 705-715 (March 1, 2004). Full text online at http://www.cdc.gov/hepatitis/PDFs/fiore_ha_transmitted_by_food.pdf.
[5] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1.
[6] Id.
[7] Fiore, Anthony, Division of Viral Hepatitis, CDC, “Hepatitis A Transmitted by Food,” supra note 7; Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[8] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1.
[9] Id.; See also Jaykus Lee Ann, “Epidemiology and Detection as Options for Control of Viral and Parasitic Foodborne Disease,” Emerging Infectious Diseases, Vol. 3, No. 4, pp. 529-39 (October-December 1997). Full text of the article is available online at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2640072/pdf/9366607.pdf
[10] Fiore, Anthony, supra note 7; CDC, “Hepatitis A,” supra note 5; See also CDC, “Surveillance for Acute Viral Hepatitis – United States, 2007, Morbidity and Mortality Weekly Report, Surveillance Summaries, Vol. 58, No. SS03 (May 22, 2009) at http://www.cdc.gov/mmwr/preview/mmwrhtml/ss5803a1.htm.
[11] Fiore, Anthony, Division of Viral Hepatitis, CDC, “Hepatitis A Transmitted by Food,” supra note 7.
[12] Lin, K. Y., & Fang, C. T. (2021). Public health responses to person-to-person hepatitis A outbreaks. The Journal of Infectious Diseases, 223(3), 359-361.
[13] Hofmeister, M. G., Xing, J., Foster, M. A., Augustine, R. J., Burkholder, C., Collins, J., … & Spradling, P. R. (2021). Hepatitis A person-to-person outbreaks: Epidemiology, morbidity burden, and factors associated with hospitalization—Multiple States, 2016–2019. The Journal of Infectious Diseases, 223(3), 426-434.
[14] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1; Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[15] CDC, “Updated recommendations from Advisory Committee on Immunization Practices (ACIP) for use of hepatitis A vaccine in close contacts of newly arriving international adoptees,” Morbidity and Mortality Weekly Report, Vol. 58, No. 36, (Sept. 18, 2006), http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5836a4.htm; Fiore, Anthony, et al., Advisory Committee on Immunization Practices (ACIP), Prevention of Hepatitis-A Through Active or Passive Immunization: Recommendations, Morbidity & Mortality Weekly Review, Vol. 55, Report 407, (May 29, 2006) at http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5507a1.htm; Todd, Ewan C.D., et al., “Outbreaks Where Food Workers Have Been Implicated in the Spread of Foodborne Disease. Part 6. Transmission and Survival of Pathogens in the Food Processing and Preparation-environment,” Journal of Food Protection, Vol. 72, 202-19 (2009). Full text of the article is available online at http://courses.washington.edu/eh451/articles/Todd_2009_food%20processing.pdf.
[16] Fiore, Anthony, Division of Viral Hepatitis, CDC, “Hepatitis A Transmitted by Food,” supra note 7.
[17] Fiore, Anthony, Division of Viral Hepatitis, CDC, “Hepatitis A Transmitted by Food,” supra note 7
[18] Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[19] CDC, “Hepatitis A,” supra note 5; Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1
[20] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1
[21] Id.
[22] Id.; See also Sagliocca, Luciano, et al., “Efficacy of Hepatitis A Vaccine in Prevention of Secondary Hepatitis A Infection: A Randomized Trial,” Lancet, Vol. 353, 1136-39 (1999). Abstract at http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(98)08139-2/abstract.
[23] CDC, “Hepatitis A,” supra note 5.
[24] Id.: See also Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1; Fiore, Anthony, Division of Viral Hepatitis, CDC, “Hepatitis A Transmitted by Food,” supra note 7.
[25] CDC, “Hepatitis A,” supra note 5; Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1; Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[26] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1; Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[27] Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[28] CDC, “Hepatitis A,” supra note 5; Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1; Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[29] Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[30] Fiore, Anthony, et al., Advisory Committee on Immunization Practices (ACIP), Prevention of Hepatitis-A Through Active or Passive Immunization: Recommendations,” supra note 20; Gilkson Miryam, et al., “Relapsing Hepatitis A. Review of 14 cases and literature survey,” Medicine, Vol. 71, No. 1, 14-23 (Jan. 1992). Abstract of article online at http://www.ncbi.nlm.nih.gov/pubmed/1312659.
[31] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1.
[32] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1; Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[33] CDC, “Hepatitis A,” supra note 5; Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[34] Gilkson Miryam, et al., “Relapsing Hepatitis A. Review of 14 cases and literature survey,” supra note 37.
[35] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1; Gilkson Miryam, et al., “Relapsing Hepatitis A. Review of 14 cases and literature survey,” supra note 37.
[36] Mayo Clinic Staff, “Hepatitis A,” supra note 1.
[37] CDC Summary, “Disease Burden from Viral Hepatitis A, B and C in the United States, 2004-2009, at http://www.cdc.gov/hepatitis/pdfs/disease_burden.pdf; CDC, “Hepatitis A,” supra note 5.
[38] Detry, Oliver, et al., “Brain Edema and Intracranial Hypertension in Fulminant Hepatic Failure: Pathophysiology and Management,” World Journal of Gastroenterology, Vol. 12, No. 46 pp. 7405-7412 (Dec. 14, 2006). Full article is available online at http://www.wjgnet.com/1007-9327/12/7405.pdf.
[39] Taylor, Ryan, et al., “Fulminant Hepatitis A Virus Infection in the United States: Incidence, Prognosis, and Outcomes,” Hepatology, Vol. 44, 1589-1597. Full text http://deepblue.lib.umich.edu/bitstream/2027.42/55879/1/21349_ftp.pdf.
[40] Id.: See also Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1.
[41] Taylor, Ryan, et. al., “Fulminant Hepatitis A Virus Infection in the United States: Incidence, Prognosis, and Outcomes,” supra note 46.
[42] Detry, Oliver, et al., “Brain Edema and Intracranial Hypertension in Fulminant Hepatic Failure: Pathophysiology and Management,” supra note 45; Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1.
[43] Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1; Schiff, E.R., “Atypical Manifestations of hepatitis-A,” supra note 23.
[44] Detry, Oliver, et al., “Brain Edema and Intracranial Hypertension in Fulminant Hepatic Failure: Pathophysiology and Management,” supra note 45.
[45] Id.; See also Taylor, Ryan, et. al., “Fulminant Hepatitis A Virus Infection in the United States: Incidence, Prognosis, and Outcomes,” supra note 46.
[46] Detry, Oliver, et al., “Brain Edema and Intracranial Hypertension in Fulminant Hepatic Failure: Pathophysiology and Management,” supra note 45; Taylor, Ryan, et. al., “Fulminant Hepatitis A Virus Infection in the United States: Incidence, Prognosis, and Outcomes,” supra note 46.
[47] Detry, Oliver, et al., “Brain Edema and Intracranial Hypertension in Fulminant Hepatic Failure: Pathophysiology and Management,” supra note 45.
[48] Detry, Oliver, et al., “Brain Edema and Intracranial Hypertension in Fulminant Hepatic Failure: Pathophysiology and Management,” supranote 45; Feinstone, Stephen and Gust, Ian, “Hepatitis A Virus,” supra note 1.
[49] Detry, Oliver, et al., “Brain Edema and Intracranial Hypertension in Fulminant Hepatic Failure: Pathophysiology and Management,” supra note 45.
[50] Detry, Oliver, et al., “Brain Edema and Intracranial Hypertension in Fulminant Hepatic Failure: Pathophysiology and Management,” supra note 45; Taylor, Ryan, et. al., “Fulminant Hepatitis A Virus Infection in the United States: Incidence, Prognosis, and Outcomes,” supra note 46.