As of Tuesday, the toll in the outbreak of E. coli O104:H4 in Germany was 3,697 illnesses, 856 cases of hemolytic uremic syndrome (HUS) and 40 deaths.
Major Shiga toxin-producing E. coli (STEC) outbreaks in the past have been transformative events for epidemiology and approaches to food safety. An hour-long conversation last Thursday with Dr. Robert V. Tauxe, deputy director, Division of Foodborne, Bacterial and Mycotic Diseases NCEZID (National Center for Emerging and Zoonotic Infectious Diseases), Centers for Disease Control and Prevention, helped put the outbreak in a broader perspective. A review of the major points follows:
DC: Would you put the German STEC E. coli outbreak in context, compared to the U.S. and other outbreaks?
RT: This is an astoundingly large and severe outbreak, particularly in regards to seriousness of health consequences.
The largest single U.S. outbreak due to STEC E. coli, in that case due to O157:H7, was the West Coast outbreak due to ground beef, hamburger, in 1993. That had 750 patients presenting with bloody diarrhea, 44 HUS cases and four deaths.
The outbreak in Germany is on a much larger scale, at least an order of magnitude worse.
The largest total number of patients in a STEC outbreak is still O157:H7 in Sakai City, Japan. This was in 1992, had over 7,000 cases, with about 121 HUS cases and three deaths. The outbreak was attributed to radish sprouts produced by one facility.
The STEC E. coli O157:H7 outbreaks have changed the way epidemiology is carried out over the last 30 years.
For example, in the U.S. we developed PulseNet, for rapid reporting and identification of dispersed clusters of E. coli, in response to the West Coast outbreak.
The Japanese developed their entire field epidemiology program in response to Sakai City. CDC helped them in their investigations, and then Dr. John Kobayashi became one of their lead consultants for developing field epidemiology. Dr. Kobayashi was the state epidemiologist for Washington state who worked with CDC on the 1993 hamburger outbreak the West Coast.
Later, the Japanese and others also started their own PulseNet system. The current outbreak may also lead to significant changes in Germany in the future.
DC: Is O104:H4 significantly more virulent, with worse health outcomes, due to being a Shiga toxin-producing STEC and an enteroaggregative strain?
RT: It’s actually not clear to me yet that O104:H4 is significantly more virulent. There were certainly a lot of severe cases. There may have been a much larger number of milder cases than was recorded, of people who were ill, but did not seek care.
DC: The German hospitals and health authorities were preparing for a second wave of patients, which might have developed from human-human disease transmission. What do you expect, now?
RT: It does not look like there will be a second wave. The number of new cases seem to be diminishing. In particular there has not been much evidence of human-to-human transmission. I have only heard of a very few possible cases, but even these were either unconfirmed or anecdotal.
DC: Wouldn’t you expect more human to human transmission with STEC in the background of enteroaggregative E. coli strains [EAEC or, in Europe, EAggEC] with their human reservoirs, not cattle, and human-to-human transmission?
RT: Now we enter into one of the more esoteric areas of E. coli knowledge and microbiology.
The enteroaggregative E. coli are much less well studied. It is more a question of how much we do not know about them as a group than predicting possible behavior of this particular STEC EAEC, based on generalizations.
EAECs have mostly been reported as causing diarrhea in children in the developing world, though they can also cause relatively mild diarrheal illness in the U.S. [1].
There can be child-to-child transmission, for example. But even concepts such as having a reservoir restricted to humans is not actually proven. It hasn’t been looked for extensively in possible animal reservoirs, so I am not confident that there isn’t one.
In addition, the EAECs are a complex of subgroups. Each subgroup, as a class, may have very different behavior.
Finally, the O104 STEC E. coli are a very rare serotype themselves, (when E. coli are categorized by their immunological or antigenic properties and classified as strains). So O104:H4 STEC may have unusual behavior even for one of the sub-groups of EAEC.
DC: How was the outbreak strain detected and characterized as an EAEC as the outbreak developed? There were a number of news reports and notifications about fast genomic characterization?
RT: The Robert Koch Institute (RKI) posted the basic descriptive markers of the outbreak strain quite early.
There are people whose whole lives are dedicated to understanding E. coli, and who could look at the basic markers and interpret them. The Shiga toxins and toxin genes were clearly there, but it was missing the markers for adherence and other factors that are usually found in normal STEC.
Instead they saw something unexpected, the adherence factor markers that are common in the EAEC strains were present.
The actual analysis of the outbreak strain as it occurred in real time was driven by classic and modern microbiology, not by determination of the whole genome sequence.
We have seen this combination of STEC and EAEC described before, although very rarely and without this kind of impact, so it was something people already knew to look for. And there have been reports of O104 strains and even of O104:H4 before.
In general, it is thought the Shiga toxins are moved by phage transfer, especially within E. coli types [2]. It could be more common a combination than we know about now.
DC: What has been the CDC’s role during the outbreak in Germany?
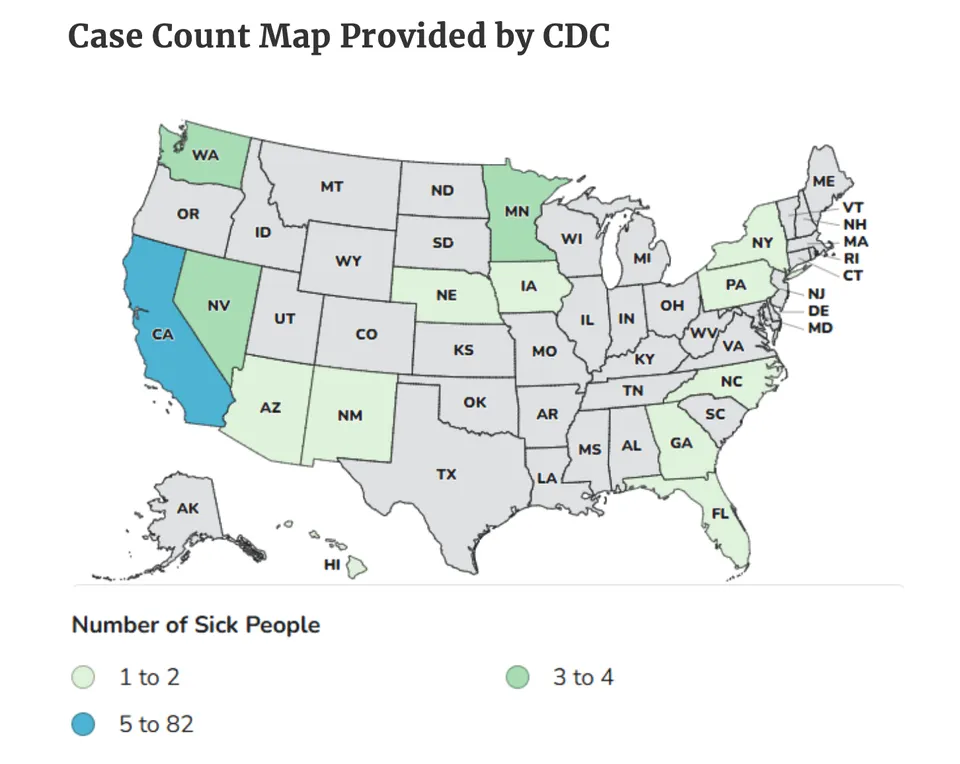
RT: When there is an outbreak in another country we contact them to offer consultation and advice, and we also offer to send an outbreak investigation team, if requested. In this case no team was sent. Our most important role was in preparing the U.S. itself, by the rapid notification and alerts to public health and other agencies in all 50 states and U.S. territories.
We did use the German investigations’ questionnaires to interview the four patients in the U.S. and return that information to them.
In general, the CDC partners with other agencies such as the FDA and USDA and state public health agencies when there is a foodborne or other outbreak in the United States. When a foodborne outbreak is within one state, that state health agency takes the lead. When it is a multistate outbreak, the CDC takes the lead.
We also take a long-term perspective on developing effective strategies for prevention, detection, and control. For example, we have worked quite hard to improve the prevention of E. coli O157:H7, on the one hand, and especially the detection and reporting as well as prevention of the non-O157:H7 STEC strains, the “non-O157’s” in shorthand.
O157:H7 is looked for routinely. So it is significant that the number of cases due to O157:H7 in the United States is down by about 50 percent, which, was included in our report in MMWR (Morbidity and Mortality Weekly Report) last week, [3] which was the annual FoodNet report card on food safety in the U.S.
At the same time as E. coli O157 is going down, the non-O157 STEC are going up, because detection is improving.
In, fa
ct, last year was the first year that the non-O157s had more cases reported than the O157s. It sounds bad, but it is good in the sense that we know we are getting more reports on the non-O157s and that people are looking for them.
We have seen significant non-O157s in the United States, of many serotypes. If a health agency hospital or other medical facility can culture stool samples in standard media, they can also do a rapid test for Shiga toxin. If this is positive, they can send the culture media on for serotyping and further identification at a state public health agency, and sometimes samples are forwarded to the CDC.
Improving the surveillance and detection for the non-O157s, in general, should also improve capacity for O104:H4. However, state public health agencies are generally stressed and facing budget cuts.
DC: You have been involved in foodborne outbreaks for a long time. How comprehensive is the association of sprouts from one farm with the whole (German) outbreak?
RT: There are three lines of very convincing evidence that seem conclusive to me.
The first comes from the epidemiological studies of large groups that ate at specific restaurants at the same time, some of whose members became ill. Field epidemiologists used the menu-directed protocols interviewing patients about which item they ordered, so patients only had to remember which meal they ate. They interviewed the restaurant managers to find out the ingredients of each menu item, and then analyzed the interview results by ingredient. The case-control odds ratios were overwhelming for sprouts as a factor, and 100 percent of ill diners had eaten sprouts.
The second line of evidence came from the trace-back efforts, that showed that this and many other affected restaurants all got their sprouts from one producer/supplier.
The third line of evidence was the consistency with a large and comprehensive national case-control study, which did find an association with sprouts, along with other salad vegetables.
In addition, there is the fact that several of the workers at the sprout farm became ill. They received sprouts for free as part of their employment. However, only one was shown to have the outbreak strain, and their illnesses came in the middle of the outbreak.
DC: So are bean sprouts the cause of the outbreak, as has been in some German press reports? And if so, which ones since any legume species could get included as ‘beans’ in translation?
RT: I think the RKI is sticking with “sprouts” for now without identifying which type of sprouts. Many of the sprouts, perhaps most of them, are sold or used in meals as mixtures of several different types of sprouts, so it would be difficult to determine which type or types of sprouts had the outbreak strain from the outbreak epidemiology alone.
Sprout production can be ideal for the multiplication of pathogens under the same conditions which are ideal for seed to sprout in. So a contamination introduced into a sprout facility can be multiplied by the sprouting process itself.
How the sprouts at this farm got contaminated is still a question. One of the possibilities is that seeds of a particular lot were contaminated. We’ve had Salmonella outbreaks due to contaminated seeds used in sprouts in the United States.
Unfortunately, it has also been shown that bacterial pathogens can last for years on or in dry seeds. How the seeds get contaminated in the first place is another question. It might happen during seed production.
The Germans are almost certainly looking at types of seeds or specific seed lots for the outbreak pathogens. But there are so many types of sprouts and therefore seeds involved, as well as particular seed lots, that this is likely to take some time.
And contamination may not have come through seeds.
DC: So as of now is there a leading suspect for the type of sprout that may have been involved based on past experience?
RT: No.
DC: Thank you for taking the time to discuss the outbreak status.
——————————————————–
[1] Under conditions of poverty and/or lack of access to medical care in developing countries, diarrheal diseases from multiple causes can lead to severe outcomes and deaths for infants and young children. In the German O104:H4 cases there is an unusual dominance of adult cases and severe outcomes due to HUS. — DC.
[2] Multiple drug resistance, characteristic of many STEC strains, can move by plasmid transfer, fairly promiscuously. — DC
(3) Vital Signs: Incidence and Trends of Infection with Pathogens Transmitted Commonly Through Food — Foodborne Diseases Active Surveillance Network, 10 U.S. Sites, 1996–2010. MMWR Weekly June 10, 2011 / 60(22);749-755.